
The Devolution of Health in England
The devolution of ‘health’ in the broadest sense is now underway in England. There are substantial structural changes being made now to the landscape of power and accountability for the commissioning and delivering of health and social care services, for improving the public’s health and for tackling the wider social determinants of health.
The Health Devolution Commission is an independent cross-party and cross-sector body working to champion and support the successful implementation of devolved and integrated NHS, public health and social care services across England. Its 2020 report ‘Building Back Health and Prosperity’ described four paradigms of health devolution (see below) in which the level of devolved freedoms to act increases as the scope of health issues to be addressed widens. The core shift it called for was to move from a paradigm of ‘health as treatment’ to a broad devolved paradigm of health that includes integrating health and social care services locally, building healthy communities and making real the connection between better health and economic prosperity.
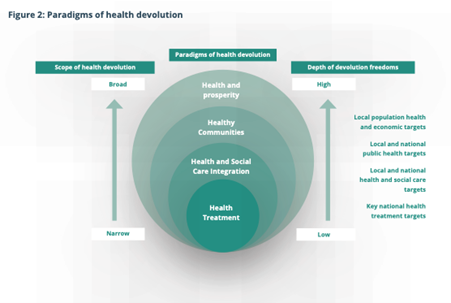
Diagram source: Building Back Health and Prosperity, The Health Devolution Commission, 2020
This fundamental shift is now becoming apparent not only in the government’s recent call for major policy shifts in the NHS Ten year Plan – from treatment to prevention, and from hospital to community – but also in the new health role envisaged for strategic authorities in the England Devolution and Community Empowerment Bill (the devolution bill).
The devolution bill places a new duty on Strategic Authorities (known as Combined Authorities and led in many places by directly elected Mayors) to ‘have regard’ to the need to i) improve the health of the people living in their areas and ii) reduce health inequalities between the people living in their areas, in the exercise of their functions. The new duty is intended to support Strategic Authorities to take action on the wider determinants of health through the delivery of their existing functions, to promote a ‘health in all policies’ approach in line with the Mission Government approach and to give Strategic Authorities a statutory locus to be active leaders for health.
The devolution bill is intended to support delivery of the Government’s aim to “tackle the social determinants of health, halving the gap in healthy life expectancy between the richest and poorest regions in England”. This approach very much echoes the analysis and call to action on health improvement by Professor Sir Michael Marmot in 2010, and now being enacted through the creation of ‘Marmot’ cities and regions throughout the UK.
For the NHS itself, the NHS Ten Year Plan published in 2025 also reflects a paradigm shift in health. It describes a new ‘devolved and diverse’ NHS operating model with an architecture (see below) that ‘supports rather than impedes the redistribution of power from the centre to the frontline’. The Plan includes a ‘commitment to earned autonomy and meaningful devolution’ with structural features such as 21 Integrated Care Boards whose footprints will eventually become coterminous with strategic authorities and required to work in partnership with their Mayor, new ‘prevention demonstrator’ partnerships such as Greater Manchester’s Live Well programme, Regional Health Innovation Zones, and most locally of all, a new Neighbourhood Health Service model.

Diagram source: NHS England guidance on the new operating model, Fit for the Future, 10 year Health Plan for England, NHS, 2025
NHSE is being merged into DHSC to create a smaller centre, with seven NHS regions. The centre’s new roles are setting strategy and forming new partnerships to deliver change; with the regions being responsible, alongside the national headquarters, for performance management and oversight of providers. Integrated Care Boards (ICBs) will be strategic commissioners of local health services, responsible for all but the most specialised commissioning using multi-year budgets.
A crucial devolution feature is the development of a Neighbourhood Health Service model within the National Health Service. ICBs will be responsible for commissioning the best, most appropriate neighbourhood providers in their footprint. A neighbourhood health plan will be drawn up by local government, the NHS and its partners at single or upper tier authority level under the leadership of the Health and Wellbeing Board, incorporating public health, social care, and the Better Care Fund. Crucially, the plans should be developed through a process of co-production with people with lived experience of the health and social care services. The ICB will bring together these local neighbourhood health plans into a population health improvement plan for their footprint and use it to inform their commissioning decisions.
In social care, the Government has commissioned Louise Casey to bring forward proposals for the development of a National Care Service. However, it is clear that this reform is about setting national standards for social care and not ‘nationalisation’ of social care services. Indeed, the decision to remove the ring-fence on central government social care grants and funding to local authorities allowing greater local flexibility on priorities and budgets for council services can be viewed as a ‘devolutionary’ approach that shifts decision-making power on social care spending from the national to the local. The decision by the government to also publish a ‘notional allocation’ of the spending on social care that each local authority could be expected (but not mandated) to make suggests that it is to local communities and the local electorate to whom councils should be accountable for the balance of their total spending power that is given to social care.
Finally, England’s public health system is a multi-layered, shared-responsibility architecture (see below) where national bodies set strategy and manage risks, NHS regional systems coordinate healthcare integration, mayoral strategic authorities address a ‘health in all policies’ approach, local authorities lead prevention and inequality reduction, and neighbourhood providers plan and deliver services directly to communities.
| Level | Primary function | Accountability |
|---|---|---|
| National | Policy, legislation, NHS leadership | DHSC/Parliament |
| NHS Regional | Coordination and NHS oversight | DHSC |
| Strategic Authority | ‘Health in all policies’ leadership, system convenor and influence | Mayoral electorate |
| Local Authority | Public health leadershipand commissioning | Council electorate |
| Neighbourhood | Service delivery and engagement | Providers and communities |
Some key questions and very live challenges now for the devolution of health in England are:
- To what extent will the devolution of power, resources and accountability in the NHS happen in practice when the traditional command-and-control culture, national NHS targets and wider political imperatives are so strong?
- To what extent will health devolution be a largely internal affair for the NHS rather than enhanced partnership working and mutual accountability at a local level between the NHS and others in local government and the voluntary sector?
- To what extent will there be new arrangements for partnership working between Strategic Authorities and Integrated Care Boards, or novel ways of working such as the Chair of the relevant ICB being nominated a deputy mayor for health?
- Should every Mayoral Strategic Authority become a Marmot place?
- To what extent will local government and the voluntary sector be equal partners with the NHS in neighbourhood health services with a broad ‘health and wellbeing’ rather than clinically-driven purpose?
- To what extent can devolution of health be rooted in the principles of co-design and co-production with patients and service users to bring about a people-centred transformation of health and social care services and systems at every level?
Social science research, including that of Professor Sir Michael Marmot, has helped to inform the initiatives and policies described herein which have got us to this point. We must now once again turn to social science to help us find answers to the questions set out above and find the solutions to the challenges we now face in the next phase of the devolution of health in England.
About the author
Phil Hope is a former British Labour Co-operative politician who was the MP for Corby from 1997 until 2010. He held several Ministerial roles during his time as an MP with responsibilities for local government, skills, charities, social enterprise and social finance. Phil was Minister of State at the Department of Health from 2008 to 2010 during which time he developed and oversaw the publication of the Social Care Green Paper, Shaping the Future of Care in July 2009. As Minister of State for Care Services his work included development of the White Paper ‘Building a National Care Service’, the National Dementia Strategy, the National Mental Health Strategy ‘New Horizons’, and the National Autism Strategy. Phil is a partner in Hope Consultancy and Training that works with health and social care organisations to navigate and work with the changing geography of power in the health and care landscape.
Image credit: Adhy Savala on Unsplash